
Printable Influenza Vaccine Consent Form, Shingles Vaccine Administration Consent Form Edit Fill Sign Online Handypdf
Printable influenza vaccine consent form Indeed recently has been sought by users around us, perhaps one of you. Individuals are now accustomed to using the internet in gadgets to see image and video data for inspiration, and according to the name of this article I will discuss about Printable Influenza Vaccine Consent Form.
- Forms
- Https Encrypted Tbn0 Gstatic Com Images Q Tbn 3aand9gcrmrkktiwlykahsb3jswi706t5heqbph8tklclaewalal7 Tu Usqp Cau
- Document 13231815
- Free Consent Form Template Sample Pdf Word Eforms Free Fillable Forms
- Flu Vaccine Consent Form Template
- Https Www Chesco Org Documentcenter View 59610 Flu Vaccine Consent English 2020
Find, Read, And Discover Printable Influenza Vaccine Consent Form, Such Us:
- Print Materials Cdc
- Https Encrypted Tbn0 Gstatic Com Images Q Tbn 3aand9gcq2trtguxqp8d9nwoni2eqrotyehqvogenbc8sbxg2iozljpa Usqp Cau
- Free 8 Sample Vaccine Consent Form Templates In Pdf Ms Word
- Ewing New Jersey Updated Free Flu Vaccination Clinic Information And Forms
- Free Flu Shots La County Library
If you re searching for Down Syndrome Ultrasound Vs Normal 20 Weeks you've arrived at the ideal place. We have 104 images about down syndrome ultrasound vs normal 20 weeks adding pictures, photos, photographs, wallpapers, and more. In such web page, we also have number of graphics available. Such as png, jpg, animated gifs, pic art, symbol, blackandwhite, translucent, etc.
Https Www Battlinminers Com Cms Lib Pa50000138 Centricity Domain 1123 2019 20consent 20form 20pahnh 20iiv 20final Pdf Down Syndrome Ultrasound Vs Normal 20 Weeks

Walgreens Var Form Fill Out And Sign Printable Pdf Template Signnow Down Syndrome Ultrasound Vs Normal 20 Weeks
Https Immunizenevada Org Sites Default Files Trainings Immunization 20toolkit 20for 20wic 20staff 202019 20final Pdf Down Syndrome Ultrasound Vs Normal 20 Weeks
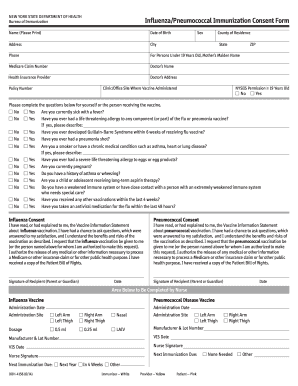
Https Www Gov Mb Ca Health Flu Docs Flupneumo Consentform Pdf Down Syndrome Ultrasound Vs Normal 20 Weeks
Doh Form 2020 Fill Out And Sign Printable Pdf Template Signnow Down Syndrome Ultrasound Vs Normal 20 Weeks

Immtrac Forms And Documents Down Syndrome Ultrasound Vs Normal 20 Weeks
Have you ever had a life threatening reaction to the influenza vaccine.

Down syndrome ultrasound vs normal 20 weeks. Screening for influenza vaccine eligibility 1. It should be signed by the patient or in the case of a minor by a parent or legal guardian. For vaccinator use only.
Date uhs mcr 60nov 2020 2021 inactivated flu vaccine consent clinicdoc vaccine information sheet 8152019. I understand the risks and benefits associated with the influenza vaccine and have had any questions satisfactorily answered. Information about the person getting vaccinated.
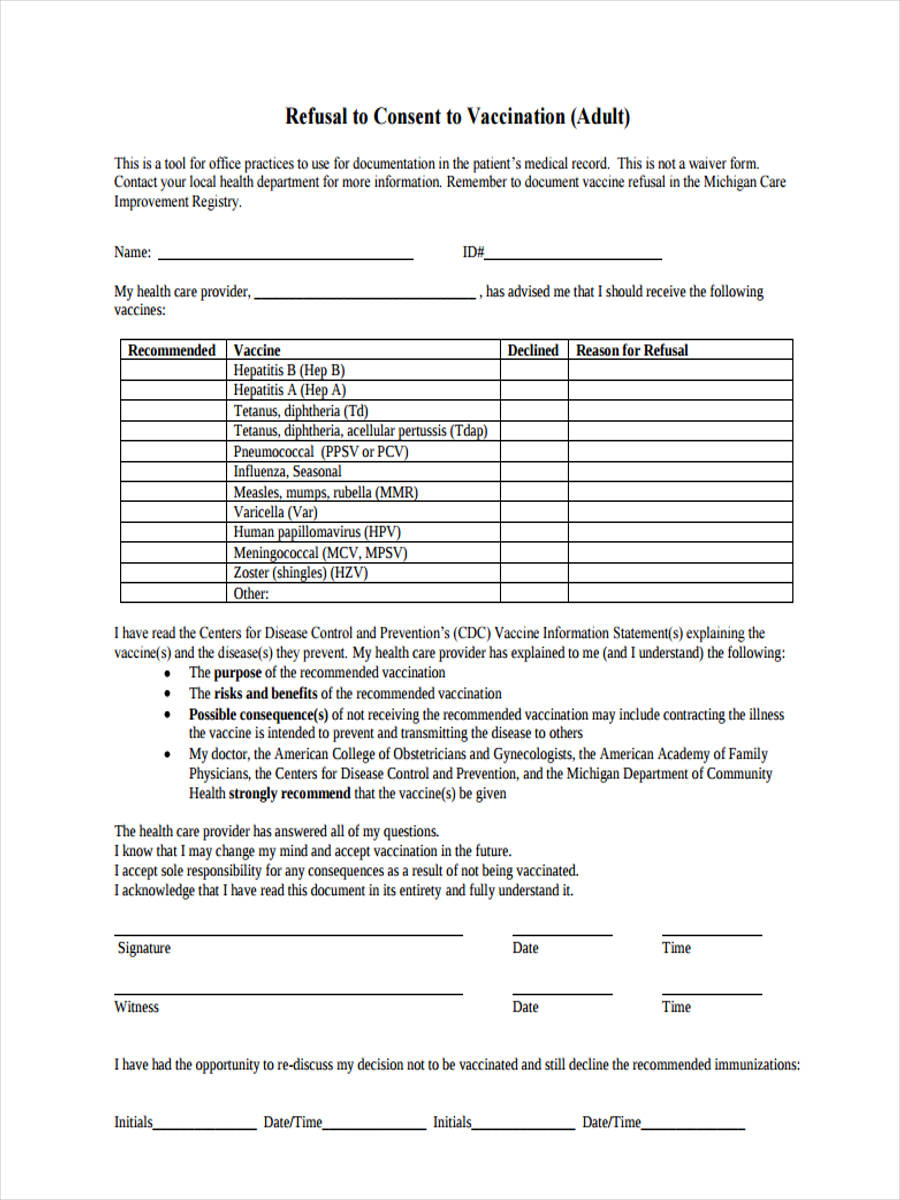
I will advise my primary healthcare provider of my vaccination. A flu shot influenza vaccine consent form is a written authorization that gives a nurse or other medical practitioner the go ahead to administer the flu vaccine. Flu vaccine form patient name.
I the undersigned have read or had explained to me the vaccine information sheet vis. Are you moderately or severely ill today. Covid screening and health information.
I understand that if i have any adverse reaction or have a question about this vaccination i will call uhs at 585 275 2662. Do you have a history of guillain barre syndrome. This form includes a series of questions that can help to exclude patients who are at risk for complications and those who otherwise.
Do you have a severe allergy to eggs. Patient full name address emergency contact emergency contact phone number physician nurse practitioner physiciannp phone number 2. 6 months and older 1.
Influenza vaccine consent form.

Free 9 Vaccine Consent Forms In Pdf Ms Word Down Syndrome Ultrasound Vs Normal 20 Weeks

Seasonal Flu Vaccine Clinic For Putnam County Sheriff S Department Down Syndrome Ultrasound Vs Normal 20 Weeks
Http Www Mcelroypharmacy Com Assets Pdf Forms Flu Vaccine Consent Pdf Down Syndrome Ultrasound Vs Normal 20 Weeks
Free 9 Vaccine Consent Forms In Pdf Ms Word Down Syndrome Ultrasound Vs Normal 20 Weeks
More From Down Syndrome Ultrasound Vs Normal 20 Weeks
- Dow Jones Industrial Average Stocks Cnn
- Downward Dog Push Up Muscles
- Influenza Vaccine Types 2019
- Pfizer Stocks History
- Indonesia Vaccine For Covid 19
Incoming Search Terms:
- Flu Shot Consent Form Region Of Peel Fill Online Printable Fillable Blank Pdffiller Indonesia Vaccine For Covid 19,
- Https Www Gov Mb Ca Health Flu Docs Flupneumo Consentform Pdf Indonesia Vaccine For Covid 19,
- Https Www Kdheks Gov Immunize Download Toolkit Fillable Resident Pneumococcal Vaccination Consent Form Pdf Indonesia Vaccine For Covid 19,
- Immunizations Hy Vee Indonesia Vaccine For Covid 19,
- Vaccine Information Statement Inactivated Influenza Vis Cdc Indonesia Vaccine For Covid 19,
- Patient Consent Form For Seasonal Influenza Vaccine Edit Fill Sign Online Handypdf Indonesia Vaccine For Covid 19,